
VIDEO
CONTENT
QUIZ
MATERIALS
Quick Facts
Key Features
Origin
Insertion
Actions
Clinical Correlates
Innervation
Arterial Supply
Quick Facts
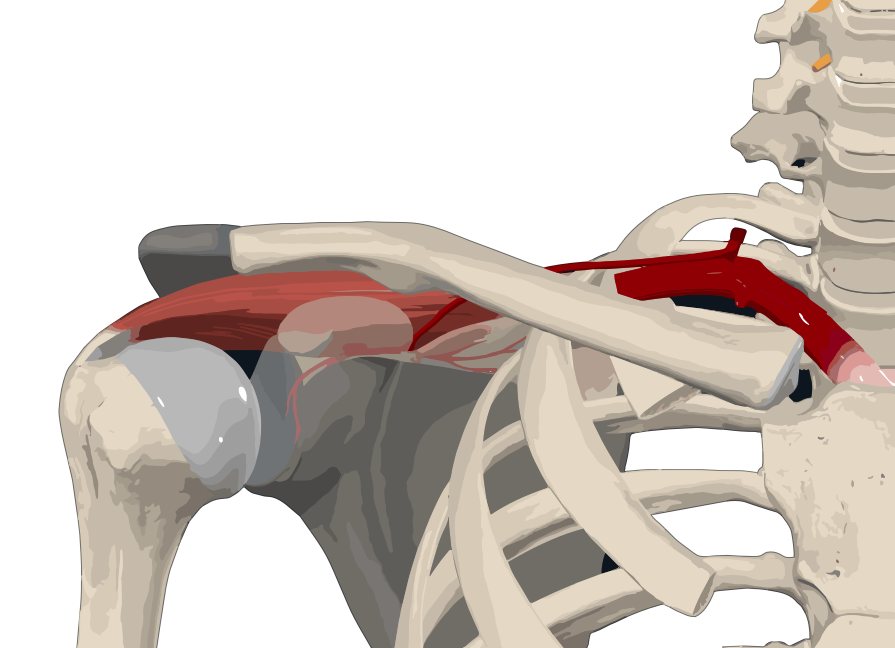
- Origin: Supraspinous fossa of scapula.
- Insertion: Greater tubercle of humerus.
- Action: Abducts and stabilizes arm at glenohumeral (shoulder) joint.
- Innervation: Suprascapular nerve (C5-C6).
- Arterial Supply: Suprascapular and dorsal scapular arteries.
Origin
- The supraspinatus muscle originates from:
- Medial two-thirds of the supraspinous fossa of the scapula.
- Internal surface of the supraspinous fascia.
Insertion
- The muscle fibers travel laterally, inserting onto the superior facet of the greater tubercle of the humerus via a thick tendon.
- Part of this tendon merges with the capsule of the glenohumeral joint.
Function: The primary function of the Supraspinatus muscle is to abduct the arm from 0 to 15 degrees, when it is the main agonist, then assists the deltoid to produce abduction beyond this range up to 90 degrees. It also plays a crucial role in stabilizing the glenohumeral (shoulder) joint by holding the head of the humerus in the glenoid fossa of the scapula during movement
Testing: The Supraspinatus muscle can be tested by moving the arm into 90 degrees of abduction in the plane of the scapula
Injury or Rupture of the Rotator Cuff
Definition and Overview
- Rotator Cuff: A group of muscles and tendons surrounding the shoulder joint, maintaining the stability and facilitating movement.
- Injury/Rupture: Can range from inflammation (tendinitis) to tears in the muscles or tendons.
Causes
- Overuse: Repetitive arm activities, especially overhead motions.
- Age: Degenerative changes in older adults.
- Trauma: Acute injuries from falls or accidents.
- Occupation/Sports: Activities requiring repetitive arm motions.
Symptoms
- Pain: Especially when lifting the arm or at night.
- Weakness: Difficulty in lifting or rotating the arm.
- Limited Mobility: Reduced range of motion in the shoulder.
- Swelling and Tenderness: Around the shoulder region.
Diagnosis
- Physical Examination: Assessing range of motion and muscle strength.
- Imaging Tests: MRI, Ultrasound, or X-rays to visualize tears or inflammation.
- Arthroscopy: Invasive procedure for a detailed view, if needed.
Treatment
- Conservative:
- Rest: Avoiding activities that aggravate symptoms.
- Physical Therapy: Strengthening and stretching exercises.
- Medications: Pain relievers and anti-inflammatory drugs.
- Surgical:
- Arthroscopic Surgery: For repairing tears.
- Open Shoulder Surgery: In more severe cases.
- Tendon Transfer: If the torn tendon is irreparable.
Prevention
- Exercise: Regular strengthening and flexibility exercises for shoulder muscles.
- Proper Technique: Using correct form during sports or occupational activities.
- Ergonomics: Adjusting workspace to reduce strain on the shoulder.
- Warm-Up: Before engaging in physical activities.
The suprascapular nerve, a mixed nerve with both sensory and motor fibers, originates from the superior trunk of the brachial plexus, specifically from the C5 and C6 spinal cord segments. It courses laterally through the posterior triangle of the neck, passing through the scapular notch to reach the posterior scapular region. Here, it innervates the supraspinatus muscle before continuing to the inferior scapular region, passing through the spinoglenoid notch. At this point, it branches to supply the glenohumeral joint and innervate the infraspinatus muscle. The nerve provides sensory innervation to the glenohumeral and acromioclavicular joints and motor innervation to the infraspinatus and supraspinatus muscles

Suprascapular artery
- Origin: Thyrocervical trunk of the subclavian artery
- Course: Laterally parallel to the clavicle, inferiorly across suprascapular notch, and deep to the inferior scapular notch
- Branches: Acromial, muscular, suprasternal, and articular branches
- Anastomosis: Thoracoacromial and posterior circumflex scapular arteries
- Supplied Structures:
- Sternocleidomastoid, supraspinatus, and infraspinatus muscles
- Scapula and clavicle
- Acromioclavicular and glenohumeral joints
- Cutaneous supply to the superior thorax and shoulder region
Dorsal Scapular Artery
- Origin: Subclavian artery or the transverse cervical artery
- Course: Laterally through the trunks of the brachial plexus to the superior angle of the scapula, then descends along the medial aspect of the scapula
- Branches: Muscular, cutaneous, and anastomotic branches
- Anastomosis: Suprascapular, subscapular, and the upper posterior intercostal arteries
- Supplied Structures:
- Rhomboid muscles
- Latissimus dorsi muscle
- Ascending part of the trapezius muscle
- Scalenus anterior muscle
- Skin overlying the ascending part of the trapezius muscle

