
VIDEO
CONTENT
QUIZ
MATERIALS
Quick Facts
Key Features
Origin
Insertion
Actions
Clinical Correlates
Innervation
Arterial Supply
Quick Facts: Biceps Brachii Muscle
The biceps brachii is a prominent muscle in the upper arm, known for its role in forearm supination and elbow flexion. Below is a concise overview of its anatomical features and functions.
Origin
- Supraglenoid Tubercle of Scapula: One point of origin.
- Apex of Coracoid Process of Scapula: Another point of origin.
Insertion
- Radial Tuberosity: Primary point of attachment.
- Antebrachial Fascia: Secondary insertion point.
Action
- Supination of Forearm: Rotates the forearm to face palm upwards.
- Flexion of Forearm at Elbow Joint: Bends the forearm towards the upper arm.
- Effective When Forearm is Supinated: Maximizes its action in this position.
Innervation
- Musculocutaneous Nerve: Receives nerve signals from this nerve.
- Nerve Roots: Innervated by the C5-C6 nerve roots.
Arterial Supply
- Brachial Artery: Provides primary blood supply.
- Anterior Circumflex Humeral Arteries: Also contributes to its blood supply.
Structure: This muscle is relatively large and thick, consisting of two parts: a short head and a long head.
Location: It is positioned on the front side of the upper arm, lying just above the brachialis and coracobrachialis muscles.
Innervation: This muscle receives its nerve supply from the musculocutaneous nerve, specifically from the spinal nerves C5, C6, and C7.
Blood Supply: The muscle is nourished by the muscular branches of the brachial artery.
Origin
- Short Head: Apex of the coracoid process of the scapula.
- Long Head: Supraglenoid tubercle of the scapula

Insertion
- General Pathway: Both heads course distally and become a confluent muscle belly before tapering across the anterior aspect of the elbow.
- Attachment Point: Radial tuberosity and the fascia of the forearm via the bicipital aponeurosis

Actions:
- Flexion and Supination: The primary functions of the biceps muscle involve bending (flexion) and outward rotation (supination) of the forearm.
- Shoulder Flexion: Additionally, the biceps brachii plays a smaller role in raising (flexing) the shoulder, particularly within the initial 30 degrees of elevation.
Testing Method: To assess the strength of the biceps muscle, perform the following test:
- The patient should be in a supine or sitting position with adequate arm support.
- The patient’s elbow should be positioned at a slight angle or at a right angle, with the forearm in a supinated (outward-facing) position.
- The examiner should apply pressure against the lower forearm in the direction of extension to evaluate the muscle’s strength.
Clinical Correlates:
- Biceps Tendinopathy: Biceps tendinopathy is a common condition affecting this muscle. It often arises due to physical trauma or repetitive activities.
- Popeye Sign: In cases where the long head tendon of the biceps ruptures, a noticeable deformity known as the “Popeye sign” can be observed.
- Treatment: Many biceps injuries can heal naturally without requiring surgery. For acute injuries, initial treatment within the first 48 to 72 hours often involves following the POLICE Principle, which stands for Protection, Optimal Loading, Ice, Compression, and Elevation. Physiotherapy is frequently necessary to aid in the muscle’s rehabilitation.
Innervation
- Primary Nerve: Musculocutaneous nerve.
- Nerve Roots: Originates from the C5, C6, and C7 nerve roots of the brachial plexus.
- Pathway: The musculocutaneous nerve runs through the coracobrachialis muscle, supplying the biceps brachii and brachialis muscles.
Clinical Significance
- Injuries and Implications: Damage to the musculocutaneous nerve can lead to weakness in elbow flexion and forearm supination.
- Diagnostic Importance: Electromyography (EMG) studies of the biceps brachii are used to assess the integrity of the musculocutaneous nerve.
- Surgical Considerations: Awareness of the nerve’s course is vital during surgical procedures in the upper arm to prevent iatrogenic injury.

Brachial Artery
The brachial artery is a vital blood vessel of the upper arm, playing a key role in supplying blood to the arm and forearm.
Origin
- Continuation from Axillary Artery: Arises at the inferior border of the teres major muscle.
Course
- Subcutaneous Pathway: Runs along the medial aspect of the arm.
- Proximal Relations: Medial to coracobrachialis, biceps brachii, and brachialis muscles.
- Distal Descent: Passes posterior to the triceps brachii muscle.
- Median Nerve Relationship: Initially lateral, then crosses anteriorly to become medial.
- Entry into Cubital Fossa: Travels deep to the bicipital aponeurosis.
- Termination: Bifurcates into the radial and ulnar arteries near the radial neck, just distal to the elbow joint.
Branches
- Deep Brachial Artery: Descends along the posterior arm.
- Nutrient Artery to Humerus: Enters the humerus near the coracobrachialis muscle’s distal attachment.
- Collateral Arteries: Superior and inferior ulnar collateral arteries to the elbow joint.
- Muscular Branches: Supply anterior arm muscles (biceps brachii, coracobrachialis, brachialis).
- Terminal Bifurcation: Produces radial and ulnar arteries.
Supplied Structures
- Bone and Muscles: Supplies humerus, biceps brachii, coracobrachialis, brachialis.
- Forearm and Hand: Provides blood to the forearm and hand through its terminal branches.
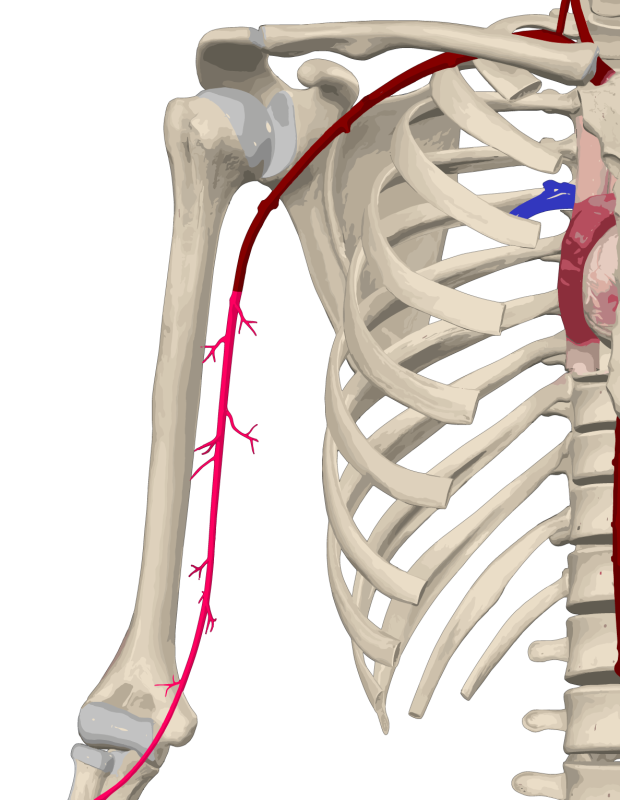
Anterior Circumflex Humeral Artery
The anterior circumflex humeral artery, a notable vessel in the shoulder region, is essential for supplying blood to the upper arm and shoulder muscles. Below is a detailed overview of its origin, course, branches, and supplied structures.
Origin
- Axillary Artery (Third Part): Arises from this segment.
- Lateral Aspect: Emerges at the level of the subscapularis muscle’s inferior border.
- Variation in Origin: In approximately 20% of individuals, it originates from a common trunk with the posterior circumflex artery.
Course
- Lateral Pathway: Moves horizontally and deep to the deltoid muscle.
- Initial Deep Positioning: Beneath the coracobrachialis and short head of the biceps brachii.
- Anterior to Humerus: Crosses the surgical neck of the humerus and the long head of the biceps brachii.
- Anastomosis with Posterior Circumflex: Wraps around the humeral neck, uniting with the posterior counterpart.
Branches
- Ascending Branch: Emerges at the intertubercular sulcus of the humerus.
- Humeral Ring Formation: Anastomoses with the posterior circumflex humeral artery.
Supplied Structures
- Muscles: Supplies the deltoid, biceps brachii, and coracobrachialis.
- Joint: Contributes to the glenohumeral joint’s blood supply.
- Bone: Nourishes the proximal humeral head.
- Skin: Supplies the area overlying the proximal humerus anteriorly.

